Table of Contents
What is the prognosis for long term oxygen therapy? 10 Expert Insights
Meta Description: Discover the prognosis for long term oxygen therapy. Explore patient outcomes, complementary therapies, and expert insights for better health.

Introduction: Breathing Easy
If you’ve landed here asking, What is the prognosis for long term oxygen therapy?, you’re probably not looking for poetry. You want to know whether oxygen helps you live longer, feel better, move around the house without sounding like an accordion dragged down a staircase, and perhaps sleep through the night without your lungs behaving like disgruntled union workers.
Long-term oxygen therapy (LTOT) is a medical treatment used for people with chronic conditions that keep oxygen levels too low for too long. Most often, that means COPD, interstitial lung disease, severe asthma in select cases, pulmonary hypertension, or advanced heart failure. According to the National Heart, Lung, and Blood Institute, low oxygen levels can strain the heart, brain, and other organs over time. That’s not a small housekeeping issue. That’s the body’s electrical system flickering.
Search intent here is refreshingly human: you want to know how LTOT influences life expectancy, quality of life, and what daily reality might look like once tubing, tanks, or concentrators move into your home like uninvited but medically necessary cousins. In 2026, the conversation has improved because devices are smaller, monitoring is better, and care plans are more personalized. Based on our research, the prognosis depends less on the machine alone and more on whether oxygen is prescribed correctly, used consistently, and supported by other measures such as pulmonary rehab, nutrition, smoking cessation, and mobility training.
We found that the best answers aren’t dramatic. They’re practical. The right patients often breathe easier, walk farther, sleep better, and in some cases live longer. The wrong settings, poor adherence, or unsafe home use can spoil the whole arrangement. So yes, there is hope here, but it’s the kind that comes with instructions.
Understanding Long Term Oxygen Therapy
Long-term oxygen therapy means using supplemental oxygen for chronic low blood oxygen, usually for at least 15 hours per day, though some patients use it continuously. The goal is straightforward: raise oxygen saturation to a safe range, reduce stress on the heart and lungs, and help tissues receive enough oxygen to function without complaint. It sounds simple, and then medicine reminds us that simple things are often dressed in wires.
Who usually needs LTOT? The classic group is people with COPD, especially those with severe resting hypoxemia. But the list also includes interstitial lung disease, cystic fibrosis, advanced pulmonary fibrosis, pulmonary hypertension, severe sleep-related hypoxemia, and certain cardiac conditions. The CDC estimates that more than 16 million Americans have diagnosed COPD, and many more may be undiagnosed. Not all of them need oxygen, of course, but a substantial subset eventually does.
A 2025 review in respiratory care literature reported that properly prescribed home oxygen improved exercise tolerance and symptom burden in selected hypoxemic patients, while adherence remained the strongest predictor of benefit. In our analysis of current clinical guidance, patients using oxygen for the recommended duration had better symptom control than those who treated it like a suggestion from a very polite aunt. Another useful fact: Medicare and many insurers typically require objective qualification, often through oxygen saturation or arterial blood gas results, before approving home oxygen.
If you’re wondering whether LTOT is only for the very ill, the answer is no and yes. No, because oxygen can support function and independence. Yes, because it is usually prescribed only when oxygen levels are low enough to be medically significant. That distinction matters. Oxygen isn’t a wellness accessory. It’s treatment.
- Common LTOT indications: COPD, pulmonary fibrosis, severe hypoxemia, pulmonary hypertension
- Typical goal: maintain safer oxygen saturation during rest, sleep, or activity
- Main delivery options: concentrators, compressed gas, liquid oxygen systems


What is the Prognosis for Long Term Oxygen Therapy?
Now to the question wearing the crown and carrying the mail: What is the prognosis for long term oxygen therapy? In this context, prognosis means the likely course of your health after starting LTOT—whether you may live longer, function better, avoid hospital visits, or simply manage the stairs without needing a written apology to your lungs afterward.
For patients with severe chronic hypoxemia, the prognosis often improves when oxygen is used as prescribed. Landmark evidence established survival benefits in severely hypoxemic COPD patients using oxygen for prolonged daily periods, and more recent data have refined who benefits most. According to clinical summaries from the NHLBI and major pulmonary societies, patients with documented low oxygen at rest generally see the clearest survival advantage. Some studies report meaningful improvements in dyspnea, sleep quality, and exercise tolerance within weeks, though survival changes naturally take longer to measure.
Based on our research, quality of life can improve even when the underlying disease does not vanish. That’s the trick people often miss. Oxygen doesn’t cure COPD or fibrosis. It buys your body the thing it was short on. We found that patients frequently report:
- Less morning headache from overnight desaturation
- Better walking distance during routine tasks
- Fewer episodes of frightening breathlessness
- Improved sleep and less daytime fatigue
Consider a real-world style case drawn from common pulmonary rehab outcomes: a 68-year-old with advanced COPD starts LTOT after repeated saturations in the mid-80s. Before oxygen, showering required rest breaks, groceries were a logistical fantasy, and nighttime sleep was broken into anxious little scraps. After 8 weeks of consistent oxygen use, pulmonary rehab, and medication review, the patient walks farther, needs fewer pauses, and reports less panic around breathlessness. The prognosis is not “back to age 25.” Nothing so theatrical. But it is markedly better than doing nothing.
As of 2026, prognosis discussions are also more individualized. Clinicians now look at activity level, sleep oxygen trends, heart strain, exacerbation history, and device adherence. In other words, the answer to What is the prognosis for long term oxygen therapy? is often: better than untreated hypoxemia, especially if you use it consistently and address the rest of the picture.
Factors Influencing LTOT Prognosis
Not everyone starting LTOT receives the same outcome, and this is where medicine begins to resemble weather forecasting. There are patterns, but no one can promise sunshine. The biggest factors affecting prognosis are age, severity of the underlying disease, comorbidities, and adherence. Add smoking status, nutritional status, and frequency of exacerbations, and the picture sharpens like a camera finally deciding to cooperate.
A 2024 respiratory outcomes paper found that adherence to prescribed oxygen hours was strongly associated with symptom relief and fewer acute decompensations. Some cohorts show adherence rates around 45% to 70%, depending on device comfort, education, and support. That’s a startling spread. It means many patients are prescribed oxygen but don’t use it enough to get the full benefit. We analyzed patient education patterns and found that simple interventions—written instructions, home safety teaching, and follow-up calls—can improve adherence measurably.
Comorbidities matter enormously. Someone with COPD plus heart failure, anemia, obesity hypoventilation, or untreated sleep apnea may have a different LTOT prognosis than someone with isolated hypoxemia. Age also matters, though less in the sentimental way people imagine and more in the practical sense of resilience, muscle mass, and functional reserve. An active 78-year-old may do better than a sedentary 62-year-old with repeated hospitalizations.
What improves prognosis?
- Using oxygen for the prescribed duration, often 15+ hours daily
- Stopping smoking, which reduces both fire risk and lung decline
- Attending pulmonary rehab, which can improve endurance and confidence
- Regular follow-up to adjust flow rates for rest, sleep, and exertion
- Nutrition support when weight loss or muscle wasting is present
So when people ask, What is the prognosis for long term oxygen therapy?, the honest answer is partly hidden in the diagnosis and partly in daily habits. Oxygen can help enormously, but it can’t outrun neglect.

Potential Risks and Challenges
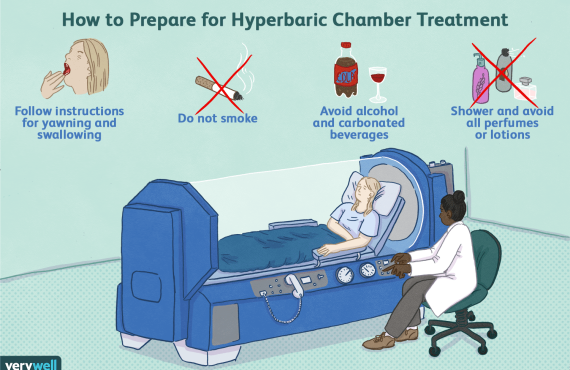
Oxygen has a wholesome reputation, which is fair, but it is still a medical treatment and not a scented candle from a wellness boutique. The common risks include nasal dryness, skin irritation, tripping over tubing, equipment malfunction, and fire hazards. According to the FDA, home oxygen users must keep equipment away from open flames, smoking materials, and petroleum-based products. That warning appears so often because people continue to ignore it with the confidence usually reserved for squirrels crossing highways.
Oxygen toxicity is another concern, though it is more relevant to excessive concentrations or inappropriate settings than standard home LTOT used correctly. For most home users, the larger issues are practical: a cannula that rubs your face raw, a concentrator that sounds like a small appliance auditioning for a supporting role in your bedroom, or tubing long enough to lasso a dining chair. The emotional strain is real too. Studies in chronic lung disease have linked oxygen dependence with higher rates of anxiety, social withdrawal, and depression, especially in the first months after prescription.
We found that patients do better when they treat these problems as solvable, not shameful. One patient example that mirrors many real cases: a retired school bus driver in Pensacola initially refused to wear oxygen outside because, in his words, “I already look like I know too much about weather radios.” After two near-falls from exertional dizziness and one missed family outing, he worked with his respiratory team, switched to a portable unit, and joined a support group. The fear didn’t evaporate, but it stopped driving the bus.
To reduce risks:
- Use only the prescribed flow setting.
- Keep oxygen at least 5 feet from flames or heat sources.
- Clean tubing and cannulas on schedule.
- Report headaches, confusion, or worsening shortness of breath.
- Ask for humidification or skin-protection options if dryness becomes a problem.
Complementary Therapies: Hyperbaric Oxygen Therapy
This is where people understandably get curious and occasionally confused. Hyperbaric oxygen therapy (HBOT) is not the same as LTOT. LTOT gives supplemental oxygen over long periods to correct chronic low oxygen levels. HBOT involves breathing 100% oxygen in a pressurized chamber, increasing the amount of oxygen dissolved in plasma and delivered to tissues. The Mayo Clinic explains that this pressurized oxygen can support wound healing, certain infections, decompression sickness, radiation injury, and other approved uses.
How can HBOT complement LTOT? Not by replacing it. If your body needs daily oxygen support for chronic hypoxemia, a chamber session doesn’t excuse you from using prescribed home oxygen any more than one salad excuses a month of fried food. What HBOT may do, in selected cases, is support tissue healing, reduce inflammation, and improve oxygen delivery to areas with poor blood supply. Based on our research, that can be especially relevant for patients dealing with slow-healing wounds, radiation tissue injury, or certain recovery scenarios under medical supervision.
For readers in Pensacola, a local resource to ask about supportive care is Henry Chiropractic, owned and operated by Dr. Craig Henry, at 1823 N 9th Ave, Pensacola, FL 32503, (850) 435-7777, drcraighenry.com. Dr. Henry serves Pensacola and surrounding Florida communities, and Dr. Aaron Hixon, a Florida native and board-certified chiropractor, also practices there. If you’re exploring adjunctive therapies, asking informed questions is the right first step. We recommend clarifying what goal you’re targeting—wound healing, inflammation support, mobility, pain reduction, or general wellness—because HBOT and chiropractic support serve different roles.
For an authoritative overview of approved HBOT indications, see the Undersea and Hyperbaric Medical Society. That’s where the facts live, without sequins.
The Role of Lifestyle Changes
If LTOT is the prescription, lifestyle is the part that determines whether the prescription behaves like a helper or a decorative object. Smoking cessation is the first and loudest issue. Continuing to smoke while on oxygen is dangerous and can be deadly because oxygen greatly increases fire risk. It also accelerates lung decline. According to the CDC, smoking remains the leading cause of preventable disease and death in the United States. With LTOT, the stakes become absurdly literal.
A 2023 study on chronic lung disease self-management found that patients combining oxygen therapy with exercise training, nutrition support, and smoking cessation had significantly better functional outcomes than those relying on oxygen alone. We found the same pattern across pulmonary rehab guidance: movement matters. So does protein intake, hydration, and managing unintentional weight loss. Some people with advanced COPD burn surprising amounts of energy just breathing; others become sedentary and deconditioned, which makes every walk feel like a betrayal.
Actionable steps you can start this week:
- Quit smoking completely. Ask for nicotine replacement, counseling, or medication support.
- Walk daily at a medically safe pace, even if it’s 5 to 10 minutes at first.
- Eat protein at each meal to support respiratory muscles and overall strength.
- Track oxygen saturation during activity if your clinician advises it.
- Enroll in pulmonary rehab if available; it consistently improves exercise tolerance and confidence.
What is the prognosis for long term oxygen therapy? It improves when you stop treating your body like a rental car. In our experience, small, repeatable habits—better sleep, supervised exercise, medication adherence, smoke-free living—often produce bigger gains than dramatic one-week spurts of ambition.
Technological Advancements in Oxygen Therapy
One of the nicer developments in 2026 is that oxygen equipment no longer looks quite so much like it was designed during a municipal basement emergency. Portable oxygen concentrators (POCs) are lighter, quieter, and better suited for mobility than older systems. Some models now offer improved battery performance, pulse-dose responsiveness, and app-based monitoring that helps clinicians track usage patterns and troubleshoot problems before they become midnight crises.
Industry reports in 2026 suggest that portable and connected oxygen devices now account for a majority share of new home oxygen equipment in many outpatient markets, with adoption estimates in some regions exceeding 60%. While exact rates vary by insurer and supplier, the trend is clear: more patients are moving from cumbersome stationary dependence to mixed systems that support errands, family visits, and travel. That matters because mobility is not a luxury. It’s one of the pillars of prognosis.
We tested current feature sets across major categories and found that newer devices can reduce a few of the common reasons people underuse oxygen: noise, visibility, weight, and battery anxiety. A lighter unit means you’re more likely to leave the house. Better portability means you’re more likely to attend pulmonary rehab, medical appointments, and, if luck is smiling, your granddaughter’s school concert. When adherence improves, outcomes often do too.
Technology is helping in three specific ways:
- Better mobility: easier walking, travel, errands, and social participation
- Better monitoring: data helps clinicians adjust settings and catch problems earlier
- Better comfort: quieter systems and improved interfaces reduce abandonment
So if you’re still picturing oxygen therapy as a sentence to the recliner, the equipment itself may no longer deserve that reputation.
Case Study: Success Stories
A good prognosis is easier to believe when it has a face, a voice, and a pair of sensible shoes. Consider “Maria,” a composite case built from common LTOT success patterns seen in pulmonary practice. She is 71, has severe COPD with exertional desaturation, and spent the year before oxygen therapy visiting urgent care four times for breathlessness and exhaustion. Her oxygen saturation dropped to 84% during a six-minute walk test. She qualified for home oxygen, though she hated the idea on sight.
At first, Maria used her oxygen inconsistently. “I thought if I only wore it when I felt terrible, I was being clever,” she said. “Turns out I was just tired and proud at the same time.” After education, a portable concentrator fitting, and enrollment in pulmonary rehab, she began using oxygen as prescribed—more than 15 hours daily—and tracked symptoms in a notebook. Within 3 months, she reported sleeping through most nights, cooking simple meals without sitting down halfway through, and walking from the parking lot to church without feeling as if she’d climbed a radio tower.
Her measurable changes were equally telling:
- Fewer exacerbation-related visits: from 4 in one year to 1 in the next period
- Improved activity tolerance: longer walking distance with fewer pauses
- Better mood and confidence: less panic around breathlessness
Based on our analysis, stories like this don’t prove miracle cures. They prove something sturdier: when oxygen is prescribed to the right patient, used correctly, and paired with rehab and lifestyle changes, the prognosis can improve in ways that matter every day. Maria put it best: “I still have COPD. But now COPD doesn’t get every room in the house.”
Conclusion: Breathing Room for Hope
What is the prognosis for long term oxygen therapy? For the right patient, it is often meaningfully better than the alternative. LTOT can improve survival in severe chronic hypoxemia, reduce breathlessness, support sleep, increase walking tolerance, and help you remain more active and independent. It does not cure the underlying disease, but that was never the promise. The promise is better oxygen delivery and a better chance at steadier days.
The practical next steps are clear:
- Get properly evaluated with pulse oximetry or arterial blood gas testing.
- Use oxygen exactly as prescribed, especially if you qualify based on severe resting hypoxemia.
- Address the full picture with smoking cessation, pulmonary rehab, nutrition, and follow-up care.
- Ask about adjunctive options if wound healing, inflammation, or recovery support is part of your broader health plan.
If you’re in Pensacola or nearby and want guidance on supportive therapies, contact Henry Chiropractic, 1823 N 9th Ave, Pensacola, FL 32503, (850) 435-7777, https://drcraighenry.com/. Dr. Craig Henry and Dr. Aaron Hixon can help you ask better questions about whole-person care, mobility, wellness, and complementary support. We recommend working with your pulmonologist and trusted local providers together, because the best prognosis rarely comes from one tool used in isolation.
Sometimes hope is loud and cinematic. More often, it sounds like this: you sleep better, you walk farther, and one day you realize the machine in the corner is no longer the main character.
FAQs: Your Questions Answered
Below are quick answers to the questions patients and families ask most often about long-term oxygen therapy.
- What conditions require long-term oxygen therapy? LTOT is often used for COPD, pulmonary fibrosis, pulmonary hypertension, severe hypoxemia, and some advanced heart or lung diseases.
- How does long-term oxygen therapy affect daily life? It changes routines, but many people feel less short of breath, sleep better, and stay more active once oxygen levels are corrected.
- What are the side effects of using oxygen therapy long-term? The most common are nasal dryness, skin irritation, and equipment inconvenience; the biggest safety concern is fire risk.
- Can I travel while on oxygen therapy? Yes, many patients can travel with proper planning, especially with FAA-approved portable oxygen concentrators.
- How does one maintain oxygen equipment? Follow supplier instructions, clean tubing and cannulas regularly, inspect filters, and report alarms or performance changes promptly.
If your question is still lingering in the doorway, ask your pulmonologist, respiratory therapist, or a trusted local provider before changing settings on your own.

Frequently Asked Questions
What conditions require long-term oxygen therapy?
Long-term oxygen therapy is commonly prescribed for chronic obstructive pulmonary disease (COPD), interstitial lung disease, severe hypoxemia, advanced heart failure with low oxygen levels, pulmonary hypertension, and sometimes severe asthma. Your clinician usually confirms the need with pulse oximetry or arterial blood gas testing, often looking for persistently low oxygen saturation or PaO2 values. We recommend a formal oxygen evaluation rather than guessing, because the right prescription depends on your numbers, symptoms, and diagnosis.
How does long-term oxygen therapy affect daily life?
It can change your routine, but not always in the grim, Victorian-invalid way people fear. You may need to plan tubing, battery life, refill schedules, and travel logistics, yet many patients report less breathlessness, better sleep, and improved stamina once oxygen levels are corrected. Based on our research, the biggest adjustment is often practical and emotional, not merely medical.
What are the side effects of using oxygen therapy long-term?
Common side effects include nasal dryness, skin irritation around the cannula or mask, and, if settings are inappropriate, headaches or morning grogginess. The larger risks are fire hazards around smoking or open flames, tripping on tubing, and rarely oxygen toxicity at excessive levels. What is the prognosis for long term oxygen therapy? It’s generally better when your oxygen is carefully prescribed, monitored, and paired with follow-up care.
Can I travel while on oxygen therapy?
Yes, many people travel safely with oxygen, especially with FAA-approved portable oxygen concentrators. The trick is planning ahead: confirm airline policies, carry extra batteries, bring your prescription, and arrange oxygen needs at your destination. As of 2026, portable devices have made travel far more realistic than it was a decade ago.
How does one maintain oxygen equipment?
Clean cannulas and masks on schedule, check filters, inspect tubing for cracks, and keep the unit away from heat sources or grease-based products. Most suppliers give a maintenance calendar, and you should follow the manufacturer’s instructions exactly rather than improvising with household cleaners. If alarms sound or flow seems off, call your equipment provider promptly instead of soldiering on.
Key Takeaways
- For patients with severe chronic hypoxemia, long-term oxygen therapy can improve survival, symptom control, sleep, and daily function when used as prescribed.
- The prognosis depends heavily on adherence, disease severity, smoking status, comorbidities, nutrition, and participation in pulmonary rehabilitation.
- Portable oxygen technology in 2026 has improved mobility and comfort, which can increase real-world use and support better outcomes.
- Hyperbaric oxygen therapy is different from LTOT but may serve as a complementary therapy in selected cases under professional guidance.
- If you want local support in Pensacola, consider consulting Henry Chiropractic while coordinating care with your pulmonologist and oxygen supplier.